According to the “World Health Association”, cardiovascular diseases (stroke, heart attack, atherosclerosis, heart disease, etc.) are the “leading” cause of death worldwide. And a direct link is found between elevated cholesterol levels in the blood and the development of these diseases. If you have high cholesterol - don't joke about it, you need to take action as soon as possible if you don't want to face severe consequences soon.
What is this cholesterol and why is it?
The body cannot function without cholesterol; it helps the body break down fats or lipids in the small intestines so that they can be absorbed into the bloodstream. In the liver, cholesterol combines with lipids and proteins to form complex compounds called lipoproteins.
Cholesterol is essential for cell membrane formation, hormone production, it helps digest food, contributes to the production of Vitamin D when the skin is exposed to sunlight. Cholesterol allows human cells to move and change shape (which plants cannot do because they lack cholesterol). Essentially, it is needed for the production of new cells and growth (hence the high cholesterol content in eggs!). Also, cholesterol is necessary for the production of estrogen, testosterone, progesterone, cortisol, aldosterone, and bile. And most importantly, nearly 25% of the cholesterol in your body is in the brain, it is needed for the production and maintenance of synapses, and the production of various hormones… That is why it is crucial to regulate cholesterol production in your body, rather than eliminating it… If cholesterol fails to do its job, the consequences can be very severe.
It is clear that cholesterol is one of the main substances in our body, it is vital for humans to function properly… And the body knows it! That is why the body can produce cholesterol from almost anything: carbohydrates, proteins, or fats. The process of cholesterol production in the body is quite complex (mostly occurring in the liver), so the body does not give up absorbing it from food (of animal origin), although the amount that can be absorbed from, say, meat or eggs, is greatly exaggerated today… (in reality, only about 15% of it is absorbed). “High cholesterol?” - we hear - “reduce meat and eggs!” This couldn't be further from the truth. Simply because the vast majority of cholesterol is produced in the body, not “taken” from food, the body is too smart to risk being dependent on external sources. Cholesterol is too important for the proper functioning of the body, so it produces it itself. Hard to believe? Just “google” “Vegans high cholesterol” and the theory that “fatty foods cause high cholesterol” collapses, as people who do not eat animal products at all also have problems with high cholesterol!
High cholesterol
So, where lies the problem of high cholesterol? It is clear that it is excessive production in the liver. Cholesterol norm in the body, as we all know, is very important. Excessive cholesterol levels are associated with cardiovascular diseases… Atherosclerosis, stroke, heart attack, cardiac arrhythmias, heart failure, pericarditis, coronary heart disease… Heart disease is the No.1 killer worldwide (the second is cancer, and the third leading cause of death in America and Europe is death from prescription drugs[26]!
The body has a mechanism to regulate the ratio of cholesterol. The so-called “good” cholesterol (HDL - high-density lipoproteins) removes the excess of “bad” (LDL - low-density lipoproteins) cholesterol.
Are there 2 types of cholesterol? Good (HDL) and bad (LDL) cholesterol?
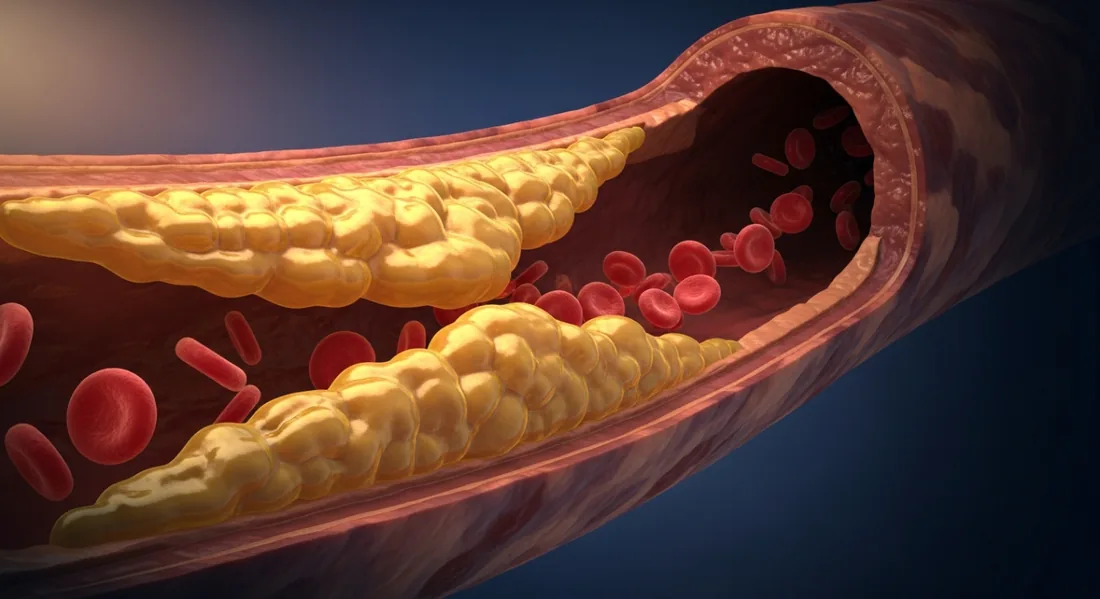
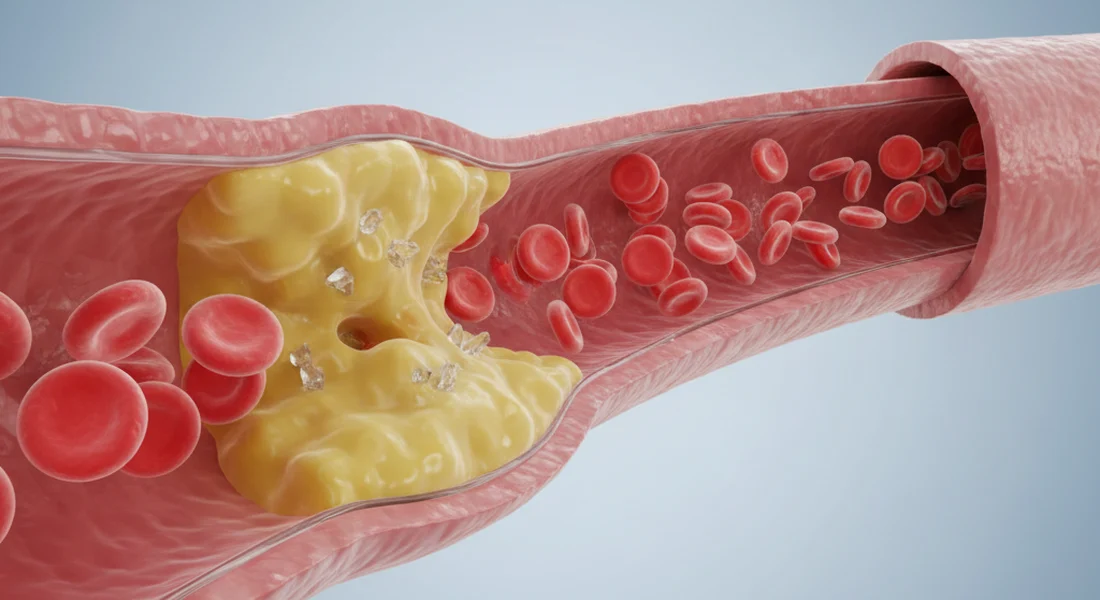
LDL cholesterol is called “bad”. Why is it called bad? It is one of the most important substances in the body, without it we would die! Excessive levels of this cholesterol are associated with coronary heart disease, heart attack, stroke, and other diseases related to blood circulation and the heart. When the artery walls are damaged (we will discuss below why), LDL cholesterol is sent to the site of damage as “repair material”. The problem arises when, due to ongoing inflammation, LDL gets stuck inside the artery wall, oxidizes, and together with immune cells forms plaques. This process, which narrows the arteries, is called atherosclerosis.
That is why, when you check your cholesterol, although LDL and total cholesterol levels are important, the HDL/LDL ratio is more important, as it shows how your body copes when cholesterol is too high. This is how the risk of heart and other circulatory problems is determined.
Cholesterol norm
At first glance, cholesterol levels in the blood can be a bit complex… Let's try to figure it out. Cholesterol is measured in millimoles per liter of blood (sometimes mg/dl).
| Total cholesterol norm | |
|---|---|
| < 5 mmol/l | Required amount |
| 5 - 6 mmol/l | Borderline |
| > 6 mmol/l | Too high |
| LDL cholesterol target (The lower the better) |
|
|---|---|
| < 1.4 mmol/l | Target for people with heart disease or high risk of heart attack |
| < 1.8 mmol/l | Target for people with heart disease or risk of heart attack |
| < 3.0 mmol/l | Target |
| > 3.0 mmol/l | High cholesterol |
| > 5.0 mmol/l | Very high cholesterol |
| HDL cholesterol target (The higher the better) |
|
|---|---|
| < 1 mmol/l (Men) < 1.2 mmol/l (Women) |
Very bad |
| 1-1.2 mmol/l (Men) 1.2-1.5 mmol/l (Women) |
Target |
| 1.6 mmol/l and above | Good |
So where does EXCESSIVE cholesterol come from?
[The] main question remains: why does your body produce too much cholesterol (we've already found out that high cholesterol doesn't "come" with food, as you're usually told)? "It's genes!" - I hear your doctor already shouting... "Yes, it's DNA!" - the big pharmaceutical companies echo. Do you really think it's your grandmother's fault? Where were the cholesterol problems, say, 300 years ago? Back then, people consumed two or three times MORE calories per day, and most of them were from animal origin... It's just the way it is, genes don't change that quickly, so the cholesterol "epidemic" (like the one now) would have existed centuries ago... (even considering that the diet was almost exclusively of animal origin). No, high cholesterol can't be inherited (except for the actual genetic disorder familial hypercholesterolemia, which, as expected, manifests in children). Do you know why it's so convenient to blame "genetics"? Because it puts you in a "you-can't-do-anything-about-it" position. You 'don't need' to exercise, 'don't need' to stop eating junk food, 'don't need' to avoid sweets and trans fats, you can calmly continue boozing beer... Just buy medication (statins), for the rest of your life! Unfortunately, few people want you to get better - a constant client for life is the best business model for a profit-seeking organization. We'll discuss the real causes of high cholesterol below. Now, let's briefly focus on statins, medications used to treat cholesterol.
Cholesterol medications (Statins)
As mentioned earlier, cholesterol is produced in the body. This synthesis is a complex process involving 30 chemical reactions. The critical moment is when, with the help of the enzyme HMG-CoA reductase, mevalonate is obtained. The enzyme HMG-CoA reductase is particularly significant because it controls whether cholesterol is produced or not... Why it receives a signal to continuously produce cholesterol will be discussed later. Since the enzyme HMG-CoA reductase is a critical controller of cholesterol synthesis, statins interfere with this reaction and block it... and voila! Cholesterol production is stopped! Blood thins, pressure drops, and you might think your problems are over... NOT REALLY, you've just created conditions for a whole chain of problems... First, cholesterol is needed for the production, maintenance, and "repair" of new cells, and now its production is blocked. Moreover, the enzyme HMG-CoA reductase, which you've successfully blocked, is also involved in other syntheses, such as vitamin A, vitamin E, vitamin K, and coenzyme Q... And so begins the whole chain of side effects.
Side effects of cholesterol medications

Most often, the active ingredient in medications that will be prescribed to you for lowering cholesterol will be “statins”… Look into their side effects (and the likelihood of their occurrence is enormous!). And you'll have to take them for the rest of your life(!?)…
Dr. Malcolm Kendrick states that the drawbacks of statins outweigh their potential benefits for many people. The prescription of statins to patients increases by almost 30% every year. So, soon everyone over 50 will have to take them. Patients should ask their doctors, "How much longer do I have to live if I take statins?" And what will be the quality of that remaining time? As studies show, statins have significant side effects that can significantly impact quality of life.
It's officially stated that statin-induced side effects can be experienced by up to 40% of users… (what?!).
Here's a survey of 4738 statin users in the Netherlands, a survey that revealed that the most common, almost 40% of all those who experienced side effects, suffered from muscle pain, and nearly a third (31%) felt joint pain. Also, 16% reported having digestive problems, and 13% experienced memory loss.
Another study revealed that patients who had definite or possible side effects from statins were not examined by their doctors, and any potential statin-related side effects were denied and not assessed for their impact on the patient's quality of life.
If you're taking statins and you're suffering from joint pain, muscle pain, liver dysfunction, digestive disorders, flushing, increased blood sugar levels, or diabetes – it could be statin-induced side effects. WARNING: if your circulatory condition is particularly "severe", sudden discontinuation of these medications can be dangerous. Try to consult with your doctor.
Unfortunately, while taking these medications, you're not getting healthier, you're just masking a severe circulatory system condition.
To this day, there hasn't been a single large-scale study of women with cardiovascular disease taking statins that would prove that statins prolong life by even one day. Moreover, the life expectancy of lower-risk women taking statins doesn't increase, and there's no prevention of heart attacks...
Side effects (from webmd.com/side-effects-of-statins):
- Headache
- Insomnia
- Skin problems
- Muscle pain, weakness
- Drowsiness
- Dizziness
- Nausea and vomiting
- Abdominal cramps or pain
- Bloating
- Diarrhea
- Constipation
- Rash
- Memory loss
- Confusion
- Increased blood sugar
- Diabetes
Let's get back to the main question…
What really determines high cholesterol
This may be completely unexpected for you, but there are numerous studies and those who search can easily find the answers. So, what determines excessive cholesterol production in your body? In short, it's sugar (glucose)!
How does this happen?
It is known that cholesterol forms atherosclerotic plaques in arteries and clogs blood vessels. However, understanding that cholesterol is a means to control inflammation and manage the damage caused by inflammation, the "system's" picture becomes obvious… Since the cause of chronic diseases is inflammation, not cholesterol [20]. The real culprit is inflammation. And what causes the most inflammation in your blood vessels? Sugar causes huge inflammation [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18]. Consuming sugar (simple carbohydrates - usually anything sweet) produces harmful compounds (AGE - Advanced glycation end products) in the body. They form when fats or proteins bind with sugar in the blood. AGE causes oxidative stress and inflammation [19].
So, inflammation arises from hormone and glucose imbalance. Since inflammation damages our blood vessel walls, our body tries to "fix" the problem by producing more cholesterol in the liver and sending it to "glue" the inflammation-irritated areas in the blood vessels. Cholesterol itself is not a problem, but rather a solution to the damage caused by other reasons. The problem is inflammation, which (most often) we cause by eating sweets (the biggest enemy, but inflammation, as we know, is also caused by heated oils, hydrogenated (trans) fats (fried, deep-fried, semi-finished products, and baked goods) and other substances and chemicals).
Yes, we are used to thinking that only people with diabetes have problems with sugar, but glucose in the body activates a hormone with surprisingly interesting principles of action. It turns out that this is one of the main hormones in the body, signaling to store nutrients, reducing blood sugar levels (if it didn't, we would die immediately with such a "modern" diet), but its main function is actually a storage/growth hormone. When we have too much of it in our blood, the body gets a signal to grow, and for growth, we need new cells, and for that to happen, we need, you guessed it, - cholesterol! So, by raising blood glucose levels, we "trick" the body into thinking we need more cholesterol, and an even greater production of it begins in the liver… Dr. Georgia Ede (diagnosisdiet.com) puts it perfectly:
"… Blood glucose levels rise when we eat too many carbohydrates(!), especially processed ones with a high glycemic index. When sugar rises, the body gets a signal to activate HMG-CoA reductase [the same one blocked by statins], which then signals all cells to produce more cholesterol, even if it's not needed. This is the main reason why so many people have high cholesterol. Sugar, flour, and starch are responsible for excessive cholesterol production. That's why low-carb, low-glycemic index, or keto diets normalize cholesterol levels in the body - these diets reduce glucose levels, which reduces HMG-CoA reductase activity."
Lowering cholesterol
As mentioned earlier, for many people, taking cholesterol-lowering medications (statins) can be dangerous. The best diet in such cases is a ketogenic one. You can read more about the ketogenic diet here ketogenine.lt. Following this diet is quite challenging because the proportions of all products are the opposite of what we're used to, and it's "forced" upon us. About 80% of all calories should come from fats (good ones, not heated oils and trans fats), about 15% from proteins, and about 5% from carbohydrates only from non-root (since starch is not allowed) vegetables. These are cauliflower, broccoli, zucchini, cucumber, and all leafy vegetables. So, no porridge, buns, potatoes, bread, alcohol, fruits, flour, sugar, juices, or anything sweet. This is a quite harsh diet, suitable for severe cases. Paleo or Atkins diets are also better than not limiting carbohydrate intake at all.
How to maximally lower Your cholesterol and improve the circulatory system without using statins?
Of course, it's about medicinal mushrooms. The first generation of statins was extracted from mushrooms and had no side effects… Do you know what the biggest problem with medicinal mushrooms is? They cannot be patented (the "patent" belongs to nature), so big pharmaceutical companies cannot monopolize the market and generate huge cash flows… Let's be objective; often, natural chemical substances don't act as quickly, and patients usually need results "here and now". You take a pill, and the next day, your cholesterol is already low… Companies always try to chemically "clone" the principles of action of plant active substances, and then they can patent their "creation"… Do they want you to have side effects? Of course not, they try as hard as they can, but our bodies are not used to metabolizing unnatural, chemical substances. You understand that medicine is not an altruistic science; it's a business… A multi-billion-dollar business… And what's the goal of EVERY business? To generate/increase profit! So, what would happen if a profit-driven business suddenly, simply, and for all time, cured your high cholesterol problem? What would happen to the business? It would lose profit and go bankrupt… So, you can be sure, this won't happen soon. This is not a conspiracy theory, just an objective look at the facts.
Let's get back to medicinal mushrooms. In Asia, medicinal mushrooms have been used for centuries, while in the Western hemisphere, research on medicinal mushrooms has only been trying to "catch up" in recent decades… Studies scientifically substantiate the traditional use of medicinal mushrooms in Eastern countries and confirm their impressive, wide-ranging benefits for the human body. It appears that medicinal mushrooms have the best answers to some of the diseases that have almost become an epidemic in the 21st century. Scientists identify compounds and complex substances that have antimicrobial, antiviral, anti-tumor, antiallergic, immunity-boosting, anti-inflammatory, anti-diabetic, cholesterol-lowering, and blood circulation and heart function-improving properties.
This is also true for the mushroom Auricula Auricularia. In the East, this mushroom has been used for about 2000 years to treat sore throat and inflammation, as well as a blood tonic. Scientific studies on the medicinal properties of this mushroom have confirmed an even broader spectrum of action. These experiments [21] concluded that two glucans (active substances) isolated from this mushroom demonstrated strong anti-cancer properties when used in mice with implanted tumors.
More importantly, studies in genetically diabetic mice revealed that the polysaccharide extracted from the Auricula Auricularia mushroom had a hypoglycemic effect. Studies in which mice were fed this polysaccharide showed decreased plasma glucose and urinary glucose [22].
It is no surprise that medicinal mushrooms have properties that fight diabetes or cancer (e.g., the widely studied substance Lentinan, extracted from Shiitake mushrooms, is used to treat cancer in conjunction with chemotherapy and radiotherapy), but it is precisely the Auricula Auricularia mushroom that is characterized by a broad-spectrum effect on blood. It has been found that its active polysaccharide compounds affect blood coagulation, platelet aggregation, and thrombosis. Studies also show that extracts of these mushrooms extract are effective in reducing total blood cholesterol levels, and most importantly, it has been proven that they reduce "bad" (LDL) cholesterol levels. This was published in the International Journal of Medicinal Mushrooms [23, 24].
This study [25] also confirmed the results:
The effect of Auricula Auricularia polysaccharides on blood lipid metabolism and lipoprotein lipase activity in mice fed a cholesterol-rich diet concluded that oral administration of [A. Auricularia] polysaccharides significantly improved overall antioxidant activity, lipoprotein lipase activity, and reduced malondialdehyde [a marker of lipid peroxidation] levels, as well as atherosclerosis markers. Total cholesterol and LDL cholesterol were significantly reduced. These findings reveal the positive effect of these mushrooms as a means of treating high cholesterol.”
If you are interested in additional research and literature, you can find it at the bottom of the page.
Let's summarize the benefits of Auricula Auricularia extract:
Anti-inflammatory effect. These polysaccharides have anti-inflammatory properties, which are consistent with the traditional use of this mushroom in Eastern cultures.
Strong antioxidant effect, slowing down the aging process.
Antithrombotic effect. These polysaccharide extracts inhibit platelet aggregation and increase clotting time, in other words, they thin the blood, making it easier to "flow". The heart can more easily "pump" such blood, thus reducing pressure.
Lowers cholesterol. Studies have shown that Auricula Auricularia polysaccharides reduce total blood cholesterol, triglycerides, and bad LDL cholesterol levels in the blood, while increasing good HDL cholesterol levels.
No side effects, unless you are allergic to mushrooms.
Only water-based (not alcohol-based) dry polysaccharide extracts are used. If you want to achieve results, this is particularly important. You can find out where to buy it best at the bottom of the page.
If this medicinal mushroom is so effective, why did your doctor prescribe statins or other chemically created medications to lower your cholesterol levels? Especially considering the significant side effects that statins can cause? As mentioned earlier, naturally occurring compounds cannot be patented, so they are of no interest to large pharmaceutical companies, which are only interested in their mechanism of action… And your doctor? He or she most likely simply doesn't know that such mushrooms exist… Do you think your doctor, after a long and difficult day at work (and it's a tough job, let's be honest), still has time to study, follow, and read research? He or she simply prescribes the necessary medication according to procedure (P.S. there are good, authoritative, well-read, and dedicated specialists out there, don't "write off" your doctor right away).
- The longer the extracts are taken, the better the results (recommended for at least 3 months).
- The effect directly depends on the amount – the higher the dose, the greater the effectiveness. You need at least 1200 mg of polysaccharide extract per day.
- Side effects may occur if you are allergic to mushrooms (very rare)
- WARNING: if your circulatory condition is particularly "severe", abruptly stopping your prescribed medication (statins) can be dangerous. Try to consult with your doctor. Reducing these medications can only be done gradually, with regular blood pressure checks.
Mushroom powder in capsules (not extracts):
To achieve significant results, you would need to drink such supplements by handfuls. In this case, the amount of active ingredients we need is small. However, such mushrooms are great for seasoning dishes and are an excellent prebiotic for your gut.
Alcohol extracts:
In liquid alcohol extracts, the polysaccharides we need are insoluble. However, terpenes and alkaloids are soluble. They have anti-inflammatory and antimicrobial effects. If you are interested in this particular effect, then a liquid alcohol extract is a great choice.
Polysaccharide extracts:
Significant results in cholesterol reduction research are based on the use of polysaccharide extracts. As polysaccharides are water-soluble (not alcohol-soluble) substances. After obtaining the extract, water can be evaporated, and a dry water-based extract is obtained, which looks like the capsules you are used to.
Polysaccharide amount per day. The largest amount is needed (obviously). The higher (percentage-wise) the polysaccharide content, the more mushrooms were needed during production to extract the active ingredient from the mushroom… It can be 5%, 15%, 25% (very rarely and more). It goes without saying that 30% is 6 times more effective than 5%. You need at least 1200 mg of polysaccharide extract per day.
AURI 25 from Zenius Labs™ – an advanced formula for cholesterol control, developed based on clinical trial data.
- Auricularia auricula polysaccharide — antioxidant activity. PubMed
- Mushroom polysaccharides — lipid metabolism modulation. PubMed
- Dietary mushroom intake and cardiovascular health. PubMed
- Auricularia auricula — hypolipidemic properties. PubMed
- Polysaccharide-based cholesterol reduction mechanisms. PubMed
- Edible mushrooms — cardiovascular disease prevention. PubMed
- Beta-glucan dietary fiber and cholesterol. PubMed
- Medicinal mushrooms — cardiovascular review. PMC
- Auricularia polysaccharide — antithrombotic effects. PubMed
- Fungal polysaccharides — immunomodulatory activity. PubMed
- Auricularia auricula — hepatoprotective properties. PubMed
- Fungal polysaccharides — oxidative stress reduction. PubMed
- Dietary fiber and serum cholesterol reduction. PubMed
- Statin alternatives — natural compounds review. PubMed
- Plant sterols and cholesterol absorption. PubMed
- Mushroom extracts — lipid-lowering clinical evidence. PubMed
- Functional food compounds and dyslipidemia. PubMed
- Polysaccharide supplementation — metabolic outcomes. PubMed
- Dietary fiber — cardiovascular risk factors. PubMed
- Statin side effects — systematic review. PMC
- Auricularia polysaccharide structure and bioactivity. ScienceDirect
- Yuan Z et al. (1998) Hypoglycemic effect of A. auricula-judae. Biosci Biotechnol Biochem
- Yoona S-J et al. (2003) Anticoagulant polysaccharide from A. auricula. Thrombosis Research
- Francia C et al. (1999) Mushrooms and cardiovascular diseases. Int J Medicinal Mushrooms
- Auricularia auricula — antioxidant capacity. PubMed
- Medicinal mushrooms — therapeutic potential review. PubMed
- World Health Organization — cardiovascular disease statistics
- Natural lipid-lowering agents — clinical review. PMC
- Statin drug side effects — patient information. WebMD
- Netherlands RADAR survey — statin side effects. SpaceDoc
- American Diabetes Association
- Zhang Z et al. (2011) Auricularia polysaccharide prevents oxidative stress. Carbohydrate Polymers, 84(1), 638-648
- Chen Y et al. (2008) A. auricula polysaccharide — blood lipid metabolism. J Food Science, 73(6)
- Ikekawa T et al. (1968) Antitumor activity of edible mushroom extracts. Cancer Research, 29(3), 734-5
- Kho S et al. (2009) Antioxidant capacity of A. auricula-judae. J Medicinal Food, 12(1), 167-174
- Wu Z et al. (2010) A. auricula polysaccharides and heart enzymes. Int J Biol Macromolecules, 46(3), 284-288
- Luo G et al. (2009) Antioxidative properties of A. auricula and hawthorn. Innovative Food Science, 10(2), 215-221
- Glass CK, Witztum JL (2001) Atherosclerosis: The Road Ahead. Cell, 104(4), 503-516
- Giugliano D (2000) Dietary antioxidants for cardiovascular prevention. Nutr Metab Cardiovasc Dis, 10(1), 38-44
- Shahidi F (2004) Functional foods: health promotion and disease prevention. J Food Science, 69(5), 146-149
- Misaki A et al. (1981) Antitumor polysaccharides from A. auricula-judae. Carbohydrate Research, 92(1), 115-29
- Barclay AW et al. (2008) Glycemic index and chronic disease risk. Am J Clin Nutr, 87, 627-37
- Boden G et al. (2005) Low-carbohydrate diet on appetite and blood glucose. Annals Internal Medicine, 142
- Brownlee M (2005) Pathology of diabetic complications. Diabetes, 1615-1625
- Djoussé L, Gaziano JM (2009) Dietary cholesterol and coronary artery disease. Atheroscler Rep, 11(6), 418-22
- Eaton SB et al. (1988) Stone agers in the fast lane. Am J Med, 84, 739-749
- Esposito K et al. (2002) Inflammatory cytokines and hyperglycemia. Circulation, 106, 2067-2072
- Greco TP et al. Oxidized-LDL complexes in acute coronary syndromes. Am J Clin Path, 133, 737-743
- Halton TL et al. (2006) Low carbohydrate diet and CVD in women. NEJM, 355, 1991-2002
- Jakobsen MU et al. (2010) Carbohydrates vs saturated fatty acids. Am J Clin Nutr, 91, 1764-8
- Mente A et al. (2009) Dietary factors and coronary heart disease. Arch Internal Medicine, 169(7), 659-69
- Siri-Tarino PW et al. (2010) Saturated fat, carbohydrate, and CVD. Am J Clin Nutr
- Welsh JA et al. (2010) Caloric sweetener and dyslipidemia. JAMA, 303(15), 1490-1497
- Westman EC et al. (2007) Low-carbohydrate nutrition and metabolism. Am J Clin Nutr, 86, 276-84
- Willett W (2011) The Great Fat Debate. J Am Diet Assoc, 111(5), 660-662
- Fan L et al. (2006) Auricularia Auricula Polysaccharide Flour. Food Chemistry, 101(3), 1158-1163
- Kaliora AC et al. (2006) Dietary Antioxidant in Preventing Atherogenesis. Atherosclerosis, 187(1), 1-17
- Chen Y et al. (2010) Hypocholesterolemic Effects of Auricularia Auricula Ethanol Extract
- Yoon SJ et al. The nontoxic mushroom Auricularia auricula contains a polysaccharide with anticoagulant activity mediated by antithrombin. Thrombosis research. 2003. PubMed
- Bian C et al. A Novel Polysaccharide from Auricularia Auricula Alleviates Thrombosis Induced by Carrageenan in Mice. Molecules (Basel, Switzerland). 2022. PubMed
- Shi Q et al. Isolation, Characterization, and Antioxidant Activity of Melanin from Auricularia auricula (Agaricomycetes). International journal of medicinal mushrooms. 2023. PubMed
- Yin CM et al. Physicochemical Properties and Antioxidant Activity of Natural Melanin Extracted from the Wild Wood Ear Mushroom, Auricularia auricula (Agaricomycetes). International journal of medicinal mushrooms. 2022. PubMed
- Liu X et al. Comprehensive utilization of edible mushroom Auricularia auricula waste residue-Extraction, physicochemical properties of melanin and its antioxidant activity. Food science & nutrition. 2019. PubMed
- González-Bonilla A et al. Dietary Supplementation with Oyster Culinary-Medicinal Mushroom, Pleurotus ostreatus (Agaricomycetes), Reduces Visceral Fat and Hyperlipidemia in Inhabitants of a Rural Community in Mexico. International journal of medicinal mushrooms. 2022. PubMed
- Abrams DI et al. Antihyperlipidemic effects of Pleurotus ostreatus (oyster mushrooms) in HIV-infected individuals taking antiretroviral therapy. BMC complementary and alternative medicine. 2011. PubMed
- Belobrajdic DP et al. β-Glucan content and in vitro bile-acid binding capacity of Agaricus bisporus and Pleurotus spp. Food & function. 2024. PubMed
- Maheshwari G et al. Characterization of the Nutritional Composition of a Biotechnologically Produced Oyster Mushroom and its Physiological Effects in Obese Zucker Rats. Molecular nutrition & food research. 2020. PubMed
- Sato M et al. Long-term intake of Tamogi-take mushroom (Pleurotus cornucopiae) mitigates age-related cardiovascular dysfunction and extends healthy life expectancy. npj aging. 2025. PubMed
- Gong J et al. Efficacy and safety of sugarcane policosanol on dyslipidemia: A meta-analysis of randomized controlled trials. Molecular nutrition & food research. 2018. PubMed
- Chen JT et al. Meta-analysis of natural therapies for hyperlipidemia: plant sterols and stanols versus policosanol. Pharmacotherapy. 2005. PubMed
- Millán J et al. Effects of a nutraceutical combination containing berberine (BRB), policosanol, and red yeast rice (RYR), on lipid profile in hypercholesterolemic patients: A meta-analysis of randomised controlled trials. Clinica e investigacion en arteriosclerosis : publicacion oficial de la Sociedad Espanola de Arteriosclerosis. 2016. PubMed
- Singh DK et al. Policosanol inhibits cholesterol synthesis in hepatoma cells by activation of AMP-kinase. The Journal of pharmacology and experimental therapeutics. 2006. PubMed
- Castaño G et al. Comparison of the effects of policosanol and atorvastatin on lipid profile and platelet aggregation in patients with dyslipidaemia and type 2 diabetes mellitus. Clinical drug investigation. 2003. PubMed
- Xiong Z et al. An overview of the bioactivity of monacolin K / lovastatin. Food and chemical toxicology : an international journal published for the British Industrial Biological Research Association. 2019. PubMed
- EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA) et al. Scientific Opinion on additional scientific data related to the safety of monacolins from red yeast rice submitted pursuant to Article 8(4) of Regulation (EC) No 1925/2006. EFSA journal. European Food Safety Authority. 2025. PubMed
- Peng D et al. Original Research: The Effects of Red Yeast Rice Supplementation on Cholesterol Levels in Adults. The American journal of nursing. 2017. PubMed
- Gerards MC et al. Traditional Chinese lipid-lowering agent red yeast rice results in significant LDL reduction but safety is uncertain - a systematic review and meta-analysis. Atherosclerosis. 2015. PubMed
- Cicero AFG et al. Red Yeast Rice for the Improvement of Lipid Profiles in Mild-to-Moderate Hypercholesterolemia: A Narrative Review. Nutrients. 2023. PubMed
- Buzzelli L et al. Alternative lipid lowering strategies: State-of-the-art review of red yeast rice. Fitoterapia. 2024. PubMed
- Hermans MP et al. The antihyperlipidemic effect of a combined supplement of standardized dry extracts of amla (Emblica officinalis), walnut (Juglans regia), olive (Olea europaea) and red yeast rice (Monascus purpureus) powder: Reduction in circulatory low-density lipoprotein-cholesterol (LDL-C) and remnant cholesterol (RC) levels in patients with hypercholesterolemia. Frontiers in pharmacology. 2023. PubMed
- Sun HJ et al. Deficiency of neutral cholesterol ester hydrolase 1 (NCEH1) impairs endothelial function in diet-induced diabetic mice. Cardiovascular diabetology. 2024. PubMed
- Park C et al. Disturbed flow induces reprogramming of endothelial cells to immune-like and foam cells under hypercholesterolaemia during atherogenesis. Cardiovascular research. 2025. PubMed
- Zhang S et al. Natural products: The role and mechanism in low-density lipoprotein oxidation and atherosclerosis. Phytotherapy research : PTR. 2021. PubMed
- Wang J et al. DBZ (Danshensu Bingpian Zhi), a Novel Natural Compound Derivative, Attenuates Atherosclerosis in Apolipoprotein E-Deficient Mice. Journal of the American Heart Association. 2017. PubMed
Frequently Asked Questions
A fat-like substance every cell needs: a cell-membrane building block, and the raw material for vitamin D, bile acids, and steroid hormones including testosterone and oestrogen. The liver makes most of it; only a smaller share comes from food. So cholesterol isn't something to eliminate. The problem isn't cholesterol itself but the balance between its blood carriers and how much lodges in artery walls.
Cholesterol doesn't dissolve in blood, so it rides carrier particles (lipoproteins). Not two cholesterols, two directions. LDL carries it from the liver out to tissues; excess builds up in artery walls, which is why it's the bad cholesterol, and the rule is: lower is better. HDL carries it back to the liver for removal, the opposite direction, which is why it's the good cholesterol, and the rule reverses: higher is better.
No single number, four values. Total: below 5 mmol/l; 5–6 borderline; above 6 too high. LDL (bad): below 3.0 mmol/l, but stricter with heart disease (below 1.8) or high heart-attack risk (below 1.4); above 3.0 is high, above 5.0 very high. HDL (good): 1.0–1.2 mmol/l for men, 1.2–1.5 for women, 1.6+ good. Triglycerides: below 1.7 mmol/l. The LDL target shifts most between people, so two identical results can bring completely different advice depending on risk.
Europe reports in mmol/l; the US and most literature in mg/dL. Same values, different unit: mg/dL = mmol/l × 38.6; mmol/l = mg/dL ÷ 38.6. So total below 193 mg/dL; LDL below 116, below 70 with heart disease, below 55 at high risk. Triglycerides use a different factor (× 88.5) because the molecule is heavier, so 1.7 mmol/l is roughly 150 mg/dL.
Total, LDL and triglyceride targets are identical for both sexes. Only HDL differs, set higher for women: below 1.2 mmol/l is very poor for women vs 1.0 for men; healthy is 1.2–1.5 (women), 1.0–1.2 (men). Oestrogen keeps HDL higher, which is why many women's panels shift after menopause, a long-standing normal result rising with no change in diet or lifestyle.
Total above 6 mmol/l is too high, LDL above 5.0 very high, but one number in isolation says little. Risk is the whole picture: LDL height, HDL drop, triglycerides, and co-factors like high blood pressure, diabetes, smoking, or existing cardiovascular disease. That's why the LDL target tightens sharply after heart disease: the same 3.0 that's normal for a healthy person is a missed target after a heart attack. Cholesterol has no symptoms, so it goes unnoticed for years until a blood test. Judge raised values against the full risk profile, not one figure.
Both, but not as most assume. The liver makes the large majority, and how much depends heavily on genetics, so dietary cholesterol (eggs, for instance) affects blood levels far less than once believed. What most drives overproduction is refined carbohydrate and sugar, plus excess weight, inactivity, alcohol and smoking. Familial hypercholesterolaemia causes very high values from a young age regardless of diet. The upshot: you can eat carefully and still test poorly, and cutting dietary cholesterol isn't the same as lowering blood cholesterol.
The strongest lever isn't fat, it's refined carbohydrate and sugar (sugar, flour, bread, potatoes, sweet drinks, juice, alcohol, processed food): these push the liver to make more cholesterol and raise triglycerides. Lowering foods in research: soluble fibre (oats, barley, legumes, psyllium) binding cholesterol in the gut, plus nuts, olive oil, oily fish, and non-starchy vegetables. One limit: soluble fibre lowers LDL but doesn't raise HDL or cut triglycerides. No single food fixes all four values, so diet alone usually moves just one.
Best-evidence measures: cut refined carbohydrate and sugar, lose excess weight, exercise regularly, stop smoking, limit alcohol, raise soluble fibre. These target the cause, liver overproduction, not a single test number. Several natural compounds also have research behind them (next question), most notably medicinal mushrooms, since the first statins were themselves isolated from fungi.
Several are studied for lipid metabolism, each by a different mechanism, which is the point:
- Auricularia auricula-judae polysaccharides, on the HMG-CoA reductase pathway, the same enzymatic step statins act on.
- Pleurotus ostreatus (oyster mushroom), which naturally contains lovastatin, on LDL.
- Policosanol, long-chain aliphatic alcohols, on gut cholesterol absorption.
- Soluble fibre, binding cholesterol in the gut.
- Red yeast rice, plant sterols, berberine, each in separate pathways.
The pattern: each acts on one point. The body makes, absorbs, recycles and removes cholesterol by several parallel routes, so blocking one leaves the rest open, which is the rationale for combining them.
Statins lower LDL effectively and are prescribed for good reason, especially after a cardiovascular event. Reported side effects: muscle pain and weakness, raised liver enzymes, digestive upset, higher type-2 diabetes risk, and, more rarely, memory and concentration issues. They also deplete coenzyme Q10, needed for cellular energy. Whether an alternative fits depends entirely on risk profile: someone post-heart-attack is in a completely different position from someone slightly raised with no other risk factors.
Because cholesterol isn't made, absorbed and removed by a single route. Each compound acts on one point, and blocking one leaves the rest open, which is why a single extract usually moves one value and leaves the others flat. AURI 25 by Zenius Labs™ is built on exactly this: instead of a bigger dose of one thing, it combines actives studied in separate, parallel pathways, hitting several routes at once. The formula is designed around how its parts interact, not the property of any one. 90 capsules; 1 in the morning, 2 in the evening.